 Watch the webcast
Watch the webcast
 Take-home messages
Take-home messages
 Download summary
Download summary
 Share summary
Share summary



EAO video stream
Clinical video session
Introduction
During the European Clinical Video Session Contest, six speakers presented their clinical cases in video format. They were selected from the applications submitted from around the world. This innovative session format allowed candidates to present clinical cases through video clips, and discussed the details afterwards.
The videos can be viewed online here.
Immediate implant with guided surgery and immediate provisional crown
This case involved the replacement of a central incisor with immediate implant placement and immediate provisional crown. The whole procedure was performed using a fully digital workflow. At the time of surgery, the provisional crown did not fit properly because the temporary abutment was overcontoured, which had not been previously planned. Six weeks after surgery the patient had soft tissue inflammation and crown mobility (which was resolved by retightening the screw).
“The whole procedure was performed using a fully digital workflow.”
The final result was achieved with a screw-retained metal-ceramic crown. The speaker highlighted that the main goal of this technique was to maintain the aesthetics, instead of recreating them. It has already been shown that highly predictable results in terms of tissue stability can be achieved with this technique (Arora et al. 2017). A digital workflow can improve efficiency and reduce chair-side time. However, the speaker emphasised that careful case selection together with operator experience are the most important factors for success.
Presentation figures

Figure 1

Figure 2

Figure 3
References:
Arora H, Khzam N, Roberts D, Bruce WL, Ivanovski S. Immediate implant placement and restoration in the anterior maxilla: Tissue dimensional changes after 2-5 year follow up. Clin Implant Dent Relat Res. 2017 Aug;19(4):694-702. doi: 10.1111/cid.12487. Epub 2017 Apr 21.
The replacement of a central incisor by the root coverage VISTA technique
This video presentation showed a case involving multiple gingival recession which was treated with the vestibular incision subperiosteal tunnel access (VISTA) technique. The VISTA technique allowed for coronal advancement of the flap while protecting the soft tissue graft inside the tunnel without papillae reflection. The procedure had the following steps:
- scaling and root planning
- a vertical incision was made and a partial thickness tunnel was elevated. The dissection – always in the same plane – reached the papillae (whose bases must be detached from the inside to permit the whole flap from being coronally displaced)
- root odontoplasty
- double horizontal mattress sutures were anchored coronally with composite
- the graft material was secured inside the tunnel
- vertical incision is sutured
The literature points to a coronally advanced flap (CAF) and connective tissue graft (CTG) as the best combination to obtain root coverage and volumetric tissue gain (both around teeth and implants), but predictable results can also be obtained with the VISTA approach.
“Predictable results can also be obtained with the VISTA approach”
The speaker is currently involved in a longitudinal study to analyse the clinical results of the VISTA technique. The volumetric changes in 2D and 3D are measured by software superimposition of the pre- and post-operative scanned models. The results can be seen in the figures. Some predictive factors were identified: recession class, tooth type, gingival thickness, root prominence, recession depth and recession width.
Presentation figures

Figure 1

Figure 2

Figure 3
Figure 4

Figure 5
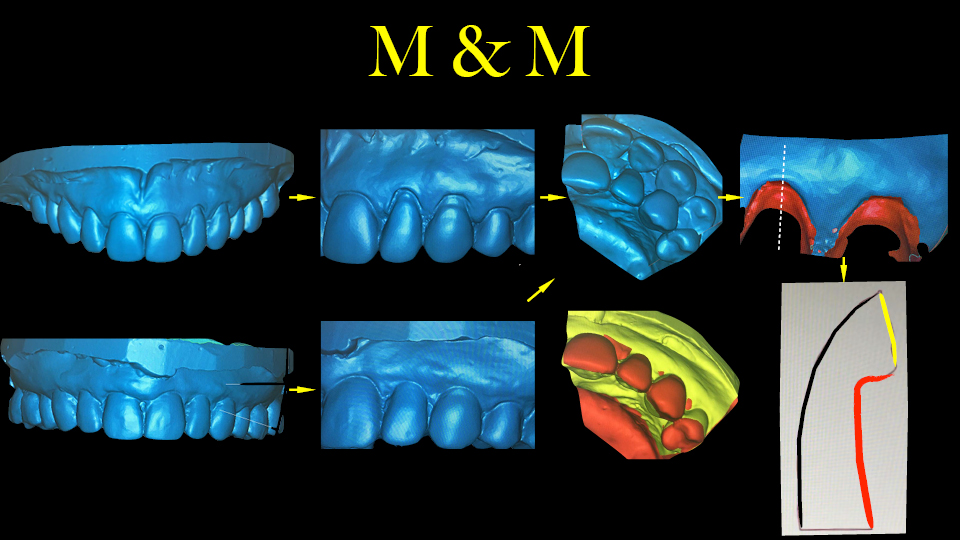
Figure 6

Figure 7

Figure 8

Figure 9
Reconstructive periodontal-plastic surgery around implant in combination with doubled-folded connective tissue graft and submarginal incisions
The speaker presented a case involving a peri-implant soft tissue dehiscence around the right upper central incisor. The treatment plan was threefold:
- Save the compromised implant
- Increase peri-implant mucosal thickness
- Improve aesthetics
In the first step, the prosthetic component was removed. A new, thinner abutment was placed without the crown. This procedure has been shown to result in better coverage (Burkhardt et al. 2008; Zucchelli et al. 2012). The second step involved multiple coronally advanced flaps after four weeks. According to Zucchelli et al. (2009), this technique compares favourably in terms of the aesthetic outcome with those approaches involving vertical releasing incisions.
“This procedure has been shown to result in better coverage”
The connective tissue graft (CTG) – regardless of its source – should be a dense tissue, rich in fibres and with as little glands or fat as possible (Studer et al. 1997; Zucchelli et al. 2010; Dellavia et al. 2014). Before detaching the graft from the palatal mucosa, the epithelium was removed. The graft was then double-folded before adapting it to the recipient site.
Before the definitive crown in was installed at 11, the left central incisor had to be extracted and an immediate implant was placed. Finally, two cemented crowns were placed at 11 and 21 and two laminate veneers at 12 and 22.
When an implant is poorly placed, a decision must be made whether to improve aesthetics by soft tissue augmentation or to remove the implant and start again from the beginning.
Presentation figures

Figure 1
References:
Burkhardt R, Joss A, Lang NP. Soft tissue dehiscence coverage around endosseous implants: a prospective cohort study. Clin Oral Implants Res. 2008 May;19(5):451-7. doi: 10.1111/j.1600-0501.2007.01497.x. Epub 2008 Mar 26.
Dellavia C, Ricci G, Pettinari L, Allievi C, Grizzi F, Gagliano N. Human palatal and tuberosity mucosa as donor sites for ridge augmentation. Int J Periodontics Restorative Dent. 2014 Mar-Apr;34(2):179-86. doi: 10.11607/prd.1929.
Studer SP, Allen EP, Rees TC, Kouba A. The thickness of masticatory mucosa in the human hard palate and tuberosity as potential donor sites for ridge augmentation procedures. J Periodontol. 1997 Feb;68(2):145-51.
Zucchelli G, Marzadori M, Mele M, Stefanini M, Montebugnoli L. Root coverage in molar teeth: a comparative controlled randomized clinical trial. J Clin Periodontol. 2012 Nov;39(11):1082-8. doi: 10.1111/jcpe.12002. Epub 2012 Sep 4.
Zucchelli G, Mele M, Mazzotti C, Marzadori M, Montebugnoli L, De Sanctis M. Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival recessions: a comparative controlled randomized clinical trial. J Periodontol. 2009 Jul;80(7):1083-94. doi: 10.1902/jop.2009.090041.
Zucchelli G, Mele M, Stefanini M, Mazzotti C, Marzadori M, Montebugnoli L, de Sanctis M. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: a comparative randomized-controlled clinical trial. J Clin Periodontol. 2010 Aug 1;37(8):728-38. doi: 10.1111/j.1600-051X.2010.01550.x. Epub 2010 Jun 24.
Sinus augmentation using an dystopic autogenous tooth
This video showed a new, economical, easy-to-harvest and completely autogenous graft material for sinus floor elevation: crushed tooth material.
The speaker showed a case involving lateral sinus elevation, where the left upper first molar was absent, the second molar was present and the third molar was included. The third molar was extracted and cut with burs. The tooth slices were then placed into a manual bone mill. The milled tooth material was then mixed with water and bone particles which had previously been collected using a bone scraper.
The procedure was as follows:
- lateral osteotomy
- the graft material was compacted
- implants were placed and the flap was sutured
- a submerged healing period of four months was observed
Two control CBCT scans were taken, one immediately after surgery and another one 12 months later. The CBCTs recorded a bone volume gain of 1.63 and 1.46 cm3 respectively.
“The clinical success rate of this procedure in 55 patients and after a seven-year follow-up period was 100%”
It is well known that dentin material and bone have a similar composition: hydroxylapatite, type I collagen and H2O. The six-month histological evaluation showed that bone formation (osteogenesis) had taken place, with enamel and dentin particles encapsulated in both sinus and alveolar ridge augmentations (Pohl et al. 2016; Pohl et al. 2017). The speaker reported that the clinical success rate of this procedure in 55 patients and after a seven-year follow-up period was 100%.
References:
Pohl V, Pohl S, Sulzbacher I, Fuerhauser R, Mailath-Pokorny G, Haas R. Alveolar Ridge Augmentation Using Dystopic Autogenous Tooth: 2-Year Results of an Open Prospective Study. Int J Oral Maxillofac Implants. 2017 July/August;32(4):870–879. doi: 10.11607/jomi.5396. Epub 2017 Jun 14.
Pohl V, Schuh C, Fischer MB, Haas R. A New Method Using Autogenous Impacted Third Molars for Sinus Augmentation to Enhance Implant Treatment: Case Series with Preliminary Results of an Open, Prospective Longitudinal Study. Int J Oral Maxillofac Implants. 2016 May-Jun;31(3):622-30. doi: 10.11607/jomi.4172.
Graftless lateral sinus floor elevation utilizing a new implant design
In this video, a new implant design was used with maxillary sinus floor elevation. The design allowed the implant threads to ‘rescue’ chips of bone from the osteotomy walls at the moment of insertion. After the Schneiderian membrane is lifted, these bone chips are pushed further into the sinus while the implant is inserted. It is hypothesised that the bone debris created by the drilling can facilitate new bone formation in the defect. Some studies on sinus floor elevation have come to this same conclusion (Dhore et al. 2008; Tabassum et al. 2009; Jungner et al. 2014).
“It is hypothesised that the bone debris created by drilling can facilitate new bone formation in the defect”
The video showed footage from the endoscopy, where it was visible how bone particles from the osteotomy attached to the implant surface and climbed along with it at the time of insertion into the sinus cavity. After the implant was placed (without grafting) the bone of the lateral bony window was replaced and ‘fixed’ with cyanoacrylate in the same position as it was before. 12-month post-op CBCT images showed bone formation around the implant, mostly around the middle third, with less around the apex.
References:
Dhore CR, Snel SJ, Jacques SV, Naert IE, Walboomers XF, Jansen JA. In vitro osteogenic potential of bone debris resulting from placement of titanium screw-type implants. Clin Oral Implants Res. 2008 Jun;19(6):606-11. doi: 10.1111/j.1600-0501.2007.01519.x. Epub 2008 Apr 16.
Jungner M, Lundqvist P, Lundgren S. A retrospective comparison of oxidized and turned implants with respect to implant survival, marginal bone level and peri-implant soft tissue conditions after at least 5 years in function. Clin Implant Dent Relat Res. 2014 Apr;16(2):230-7. doi: 10.1111/j.1708-8208.2012.00473.x. Epub 2012 Jun 21.
Tabassum A, Meijer GJ, Wolke JG, Jansen JA. Influence of the surgical technique and surface roughness on the primary stability of an implant in artificial bone with a density equivalent to maxillary bone: a laboratory study. Clin Oral Implants Res. 2009 Apr;20(4):327-32. doi: 10.1111/j.1600-0501.2008.01692.x.
Immediate implant prostheses – a guided surgery approach in anterior maxilla
The speaker began by presenting relevant scientific background for four topics related to his clinical case:
- immediate implant placement: a 2mm gap and the use of DBBM-C bone substitutes can reduce buccal plate resorption (Vignoletti & Sanz. 2014; Sanz et al. 2017)
- digital planning and guided placement: this can result in more accurate treatment than 2D planning and/or freehand placement (Schnutenhaus et al. 2018; Vercruyssen et al. 2014)
- immediate loading: although this approach shows high survival rates, it is also associated with a higher risk of failure than conventional delayed loading (Sanz-Sánchez et al. 2015). Temporary crowns can improve soft tissue maturation and are strongly recommended (Martin et al. 2014)
- digital impressions: these are already considered a valid option in single and partial implant-supported restorations (Rutkūnas et al. 2017)
The speaker then presented his case: teeth 12 to 23 were replaced with three implants at 11, 21 and 23. Both the provisional PMMA restoration and the final zirconia restorations were screw-retained.
“The digital workflow allowed a precise comparison to be made between the ‘before and after’”
The digital workflow allowed a precise comparison to be made between the ‘before and after’. The accuracy of implant placement and the volumetric changes of the soft tissue were compared by superimposing the images, giving satisfactory results.
Presentation figures

Figure 1

Figure 2

Figure 3
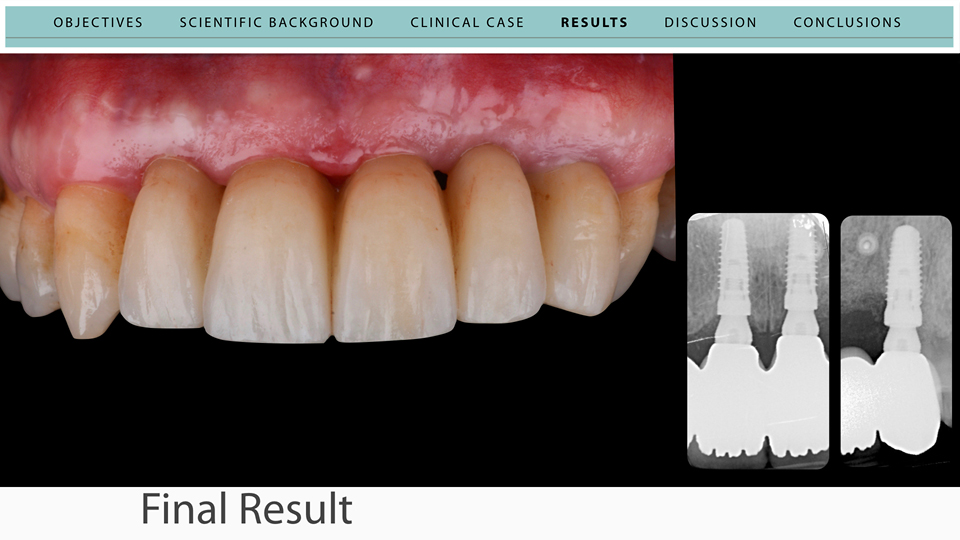
Figure 4

Figure 5
References:
Martin WC, Pollini A, Morton D. The influence of restorative procedures on esthetic outcomes in implant dentistry: a systematic review. Int J Oral Maxillofac Implants. 2014;29 Suppl:142-54. doi: 10.11607/jomi.2014suppl.g3.1.
Rutkūnas V, Gečiauskaitė A, Jegelevičius D, Vaitiekūnas M. Accuracy of digital implant impressions with intraoral scanners. A systematic review. Eur J Oral Implantol. 2017;10 Suppl 1:101-120.
Sanz M, Lindhe J, Alcaraz J, Sanz-Sanchez I, Cecchinato D. The effect of placing a bone replacement graft in the gap at immediately placed implants: a randomized clinical trial. Clin Oral Implants Res. 2017 Aug;28(8):902-910. doi: 10.1111/clr.12896. Epub 2016 Jun 7.
Sanz-Sánchez I, Sanz-Martín I, Figuero E, Sanz M. Clinical efficacy of immediate implant loading protocols compared to conventional loading depending on the type of the restoration: a systematic review. Clin Oral Implants Res. 2015 Aug;26(8):964-982. doi: 10.1111/clr.12428. Epub 2014 Jun 11.
Schnutenhaus S, Gröller S, Luthardt RG, Rudolph H. Accuracy of the match between cone beam computed tomography and model scan data in template-guided implant planning: A prospective controlled clinical study. Clin Implant Dent Relat Res. 2018 Aug;20(4):541-549. doi: 10.1111/cid.12614. Epub 2018 Apr 25.
Vercruyssen M, Cox C, Coucke W, Naert I, Jacobs R, Quirynen M. A randomized clinical trial comparing guided implant surgery (bone- or mucosa-supported) with mental navigation or the use of a pilot-drill template. J Clin Periodontol. 2014 Jul;41(7):717-23. doi: 10.1111/jcpe.12231. Epub 2014 Apr 10.
Vignoletti F, Sanz M. Immediate implants at fresh extraction sockets: from myth to reality. Periodontol 2000. 2014 Oct;66(1):132-52. doi: 10.1111/prd.12044.