 Watch the webcast
Watch the webcast
 Take-home messages
Take-home messages
 Download summary
Download summary
 Share summary
Share summary



Implant indications
Without dental implants?
Introduction
Although dental implants are widely accepted as the standard therapeutic approach for replacing missing teeth, there are a number of other options which can also be considered in our treatment planning. These approaches may be specially indicated in compromised cases, such as tooth loss in teenagers.
“We are now able to anticipate potential treatment outcomes before beginning treatment”
Thanks to advances in the field, we are now able to anticipate potential treatment outcomes before beginning treatment. When facing a new case, we should consider all possible routes and outcomes to identify the most suitable approach and achieve the planned clinical result – with or without implants. By knowing all possible approaches and weighing their pros and cons, we can identify the best therapeutic option to give the best results for each individual patient.
The future is here! CAD/CAM digital workflow in orthodontics
Replacing missing upper lateral incisors presents a clinical challenge. When a patient comes to our dental office with this problem, we have four different treatment options:
- Orthodontics
- Prosthesis
- Implants
- A combination of the above
In cases involving missing lateral incisors, space closure (when it is available) has been suggested as a more predictable treatment option in the long term from an aesthetic and periodontal point of view (Josefsson & Lindsten. 2018). Neither periodontal impairment nor temporomandibular joint dysfunction (TMD) has been reported as a result of space closure in long-term follow-ups (Rosa et al. 2016).
“It should be noted that further growth can also be expected in adults”
Compared to implant placement, a resin-bonded bridge which can later be replaced may be a good option. It should be noted that further growth can also be expected in adults, which can change the relative positions of teeth and, over time, produce infra-occlusion in implant restorations (Rosen et al. 2016).
Of the above options, implant placement has been shown to lead to the worst periodontal status after five years (Jamilian et al. 2015). This is why the replacement of missing upper lateral incisors with implants is currently debated. According to the speaker, implants should be avoided if possible in these cases.
“Implants should be avoided if possible in young patients with missing upper lateral incisors”
If we know all possible treatment options, they can be included in digital planning processes. There are tools available which let us simulate the different outcomes of treatment options using CAD-CAM technology. But the speaker asked: if CAD-CAM is so useful, fast, predictable and accurate then why is it still not common practice to incorporate it into orthodontics?
“There are tools available which let us simulate the different outcomes of treatment options using CAD-CAM technology”
The speaker described a step-by-step method for including CAD-CAM technology into orthodontic treatment.
The first step in digital planning is to apply a Digital Smile Design® (DSD) to orthodontics (where feasible) to check the different treatment options and simulate their different outcomes. This helps to inform the patient and get their consent for the chosen treatment plan (Figure 1).
Once this has been made, treatment results can be virtually planned with a combination of DSD and Invisalign® to optimise aesthetic and periodontal results. These can be shared with patients to make sure they agree with the results.
“The potential applications of CAD-CAM are not limited only to orthodontic aligners”
But the potential applications of CAD-CAM are not limited only to orthodontic aligners. Bracket treatment can be planned in this way, too. Individually customised brackets systems can be used with wires which have been pre-bent using CAD-CAM according to the computer’s virtual planning. This allows the clinician to anticipate the results before commencing treatment (Figure 2). Further, the incorporation of CBCT in the digital planning stage can also predict how difficult or complex a treatment will be (whether there is a risk of fenestration, root alignment, etc.).
Presentation figures
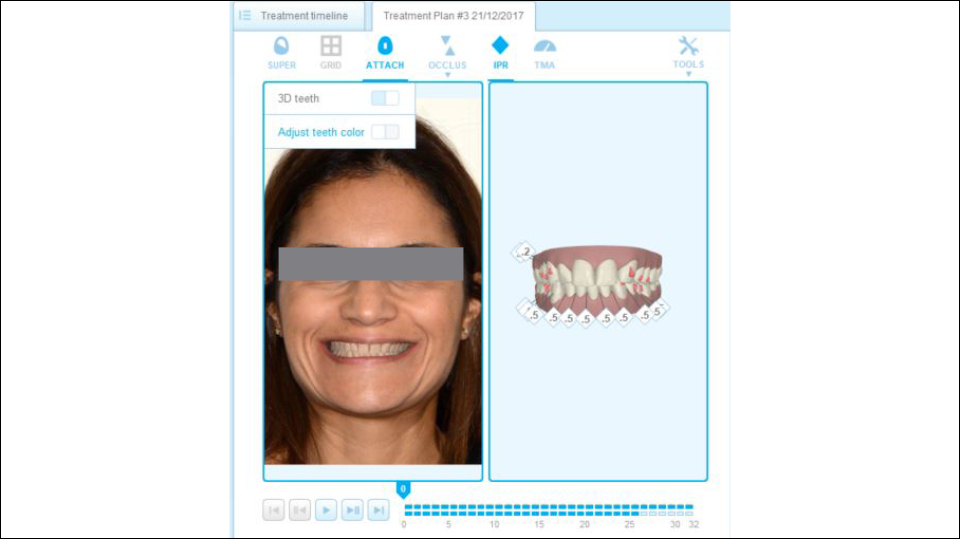
Figure 1
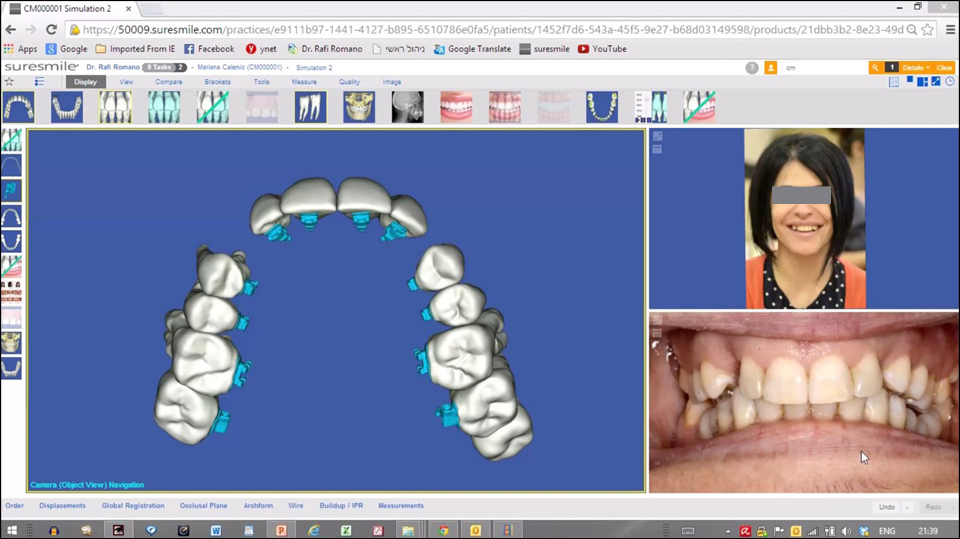
Figure 2
References:
Jamilian A, Perillo L, Rosa M. Missing upper incisors: a retrospective study of orthodontic space closure versus implant. Prog Orthod. 2015 Feb 25;16:2. doi: 10.1186/s40510-015-0072-2.
Josefsson E, Lindsten R. Treatment of missing maxillary lateral incisors: a clinical and aesthetic evaluation. Eur J Orthod. 2018 Sep 11. doi: 10.1093/ejo/cjy061. [Epub ahead of print]
Rosa M, Lucchi P, Ferrari S, Zachrisson BU, Caprioglio A. Congenitally missing maxillary lateral incisors: Long-term periodontal and functional evaluation after orthodontic space closure with first premolar intrusion and canine extrusion. Am J Orthod Dentofacial Orthop. 2016 Mar;149(3):339-48. doi: 10.1016/j.ajodo.2015.08.016.
Rosen PS, Bahat O, Froum SJ, Daftary F, Rosenthal H, Feldman S. Use of a Resin-Bonded Bridge to Replace a Congenitally Missing Lateral Incisor: Treatment of “Intrusion” of Teeth. Compend Contin Educ Dent. 2016 Jul;37(7):482-7.
Tooth transplantation
Without a doubt, osseointegration is the therapy of choice for replacing missing teeth in elderly patients. But how should an adolescent patient with anterior tooth avulsion caused by trauma be treated? In these types of cases, autotransplantation may be a useful and more reliable treatment option than implants or removable dentures.
“Osseointegration is the therapy of choice for replacing missing teeth in elderly patients”
Transplantation involves grafting a tooth from one place to another. The method has been widely used throughout the history of dental treatment. The first modern documented report of autotransplantation was published in 1992 by Jens Andreasen (Andreasen et al. 1992).
The most common indication for the procedure is replacing a non-restorable or missing first molar with an immature third molar. The second indication is transplanting premolars when anterior teeth have been lost by trauma in young patients.
When performing autotransplantation, it is crucial to avoid injuring the periodontal ligament. To this end, the immature transplanted tooth should be handled with extreme care and placed without compression in an enlarged neo-alveolus, with extra space measuring 2mm apically and 0.5–1mm all around, and should be stabilised infra-occlusally by sutures in a non-rigid way.
“When performing autotransplantation, it is crucial to avoid injuring the periodontal ligament”
The speaker outlined a proposed approach which they published in 2016 for autotransplantation using pre-planned 3D surgical guides with a fully digital workflow similar to treatments with implants (Strbac et al. 2016). The procedure is as follows: both the tooth to be extracted and the tooth to be transplanted are segmented in the 3D computer reconstruction and a virtual transplantation is made. Next, the oral scan is merged with CBCT data and a surgical template is designed and produced by 3D printing. The extraction in the recipient site is performed using a piezoelectric device to preserve the tissues as much as possible. The site is then drilled precisely through the guides for each root, and a template (with the shape of the donor tooth included) is checked to make sure the preparation is correct. Finally, the donor tooth is removed atraumatically using the piezoelectric device and immediately transplanted into the prepared site. The technique therefore draws on both surgical and guided prosthodontic procedures.
The advantages of autotransplantation are patented in cases involving children or adolescent patients, when it is indisputably the best treatment option. By using immature teeth, vitality is maintained and endodontics can be avoided, and the transplanted teeth can even be moved by orthodontics. The periodontal parameters, mobility tests and papilla indices for autotransplanted teeth are similar to natural contralateral teeth.
“The reported success rate of autotransplantation varies from 74% to 100%”
The reported success rate of autotransplantation varies from 74% to 100%. The retrospective five-year results of the speaker’s cohort study from the University of Vienna is 89.39% (Strbac et al. 2017). By using common techniques, the speaker reported that we can conclude that the success rate of autotransplanted teeth is about 90% at 5 years and 80% at 10 years.
Ankylosis and periapical lesions are a sign of autotransplantation failures and they may be strongly related to iatrogenic damage to the periodontium or press-fit compressions during intervention. For that reason, the speaker highly recommended the guided autotransplantation of teeth technique which he had previously described for treatment procedures. This technique can ensure higher success rates and reduce the risk of complications in the near future.
Presentation figures
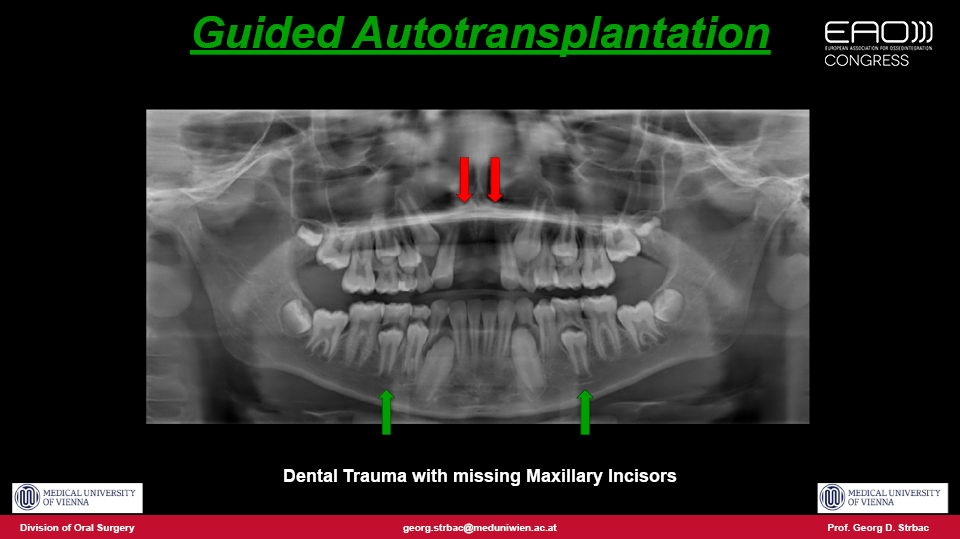
Figure 1

Figure 2
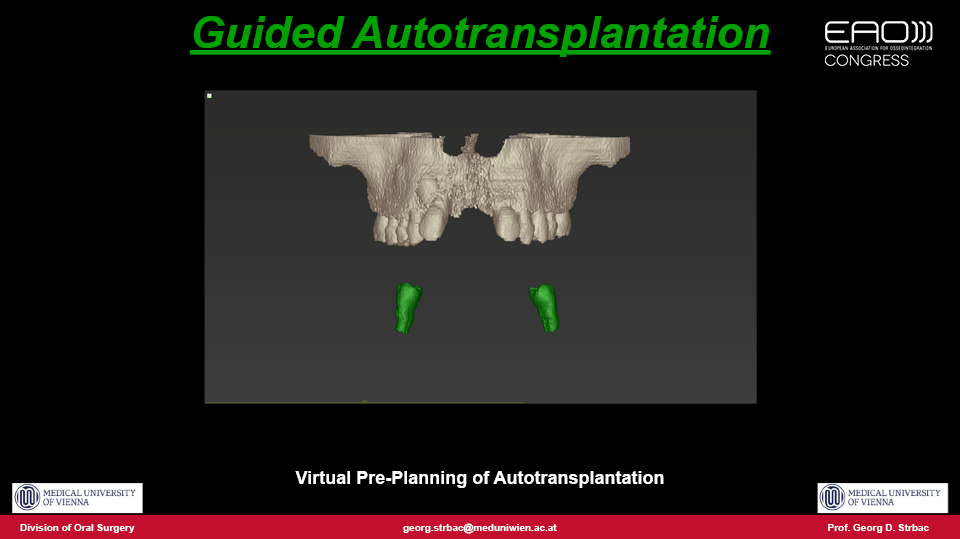
Figure 3
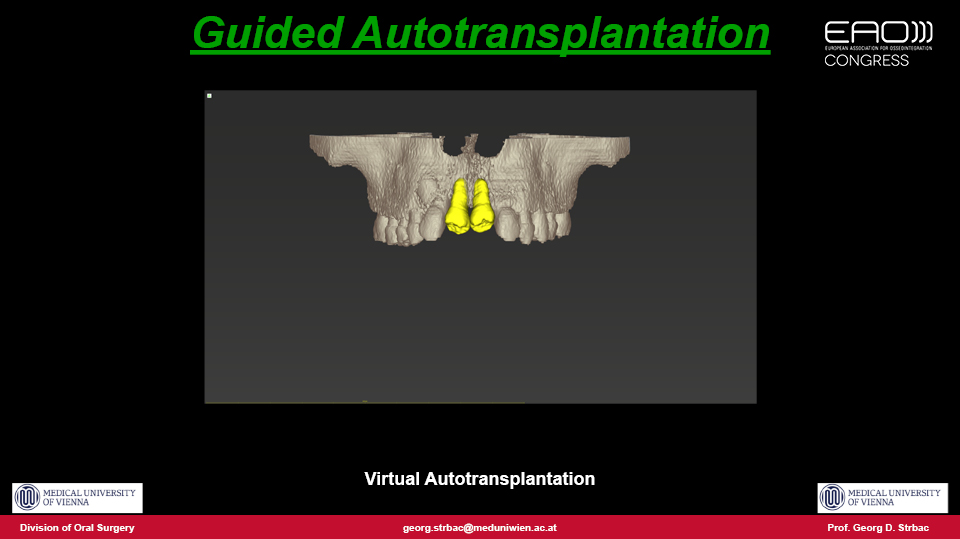
Figure 4
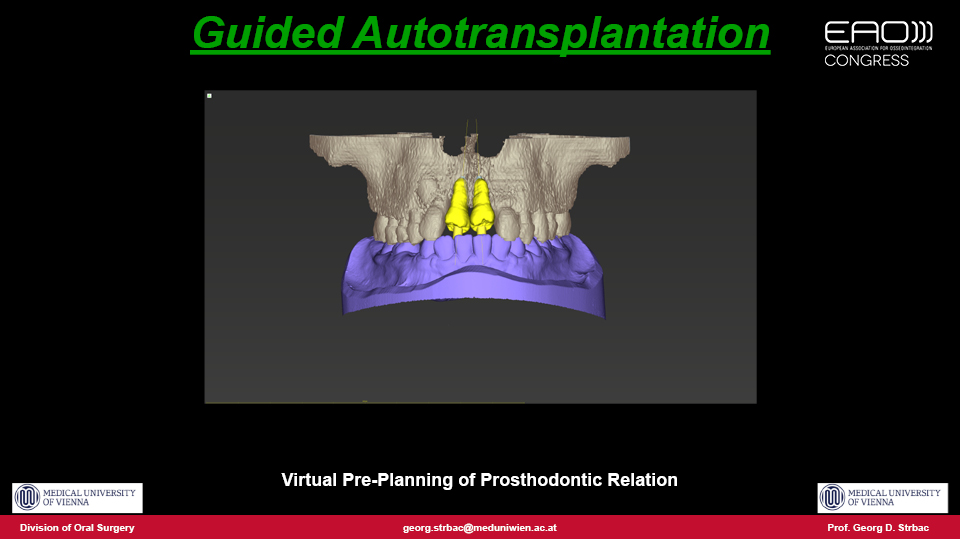
Figure 5
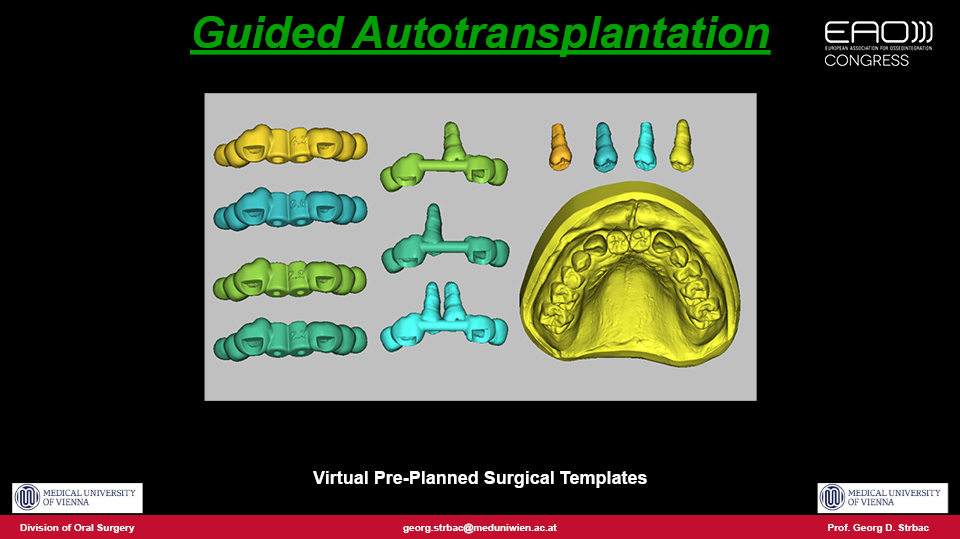
Figure 6
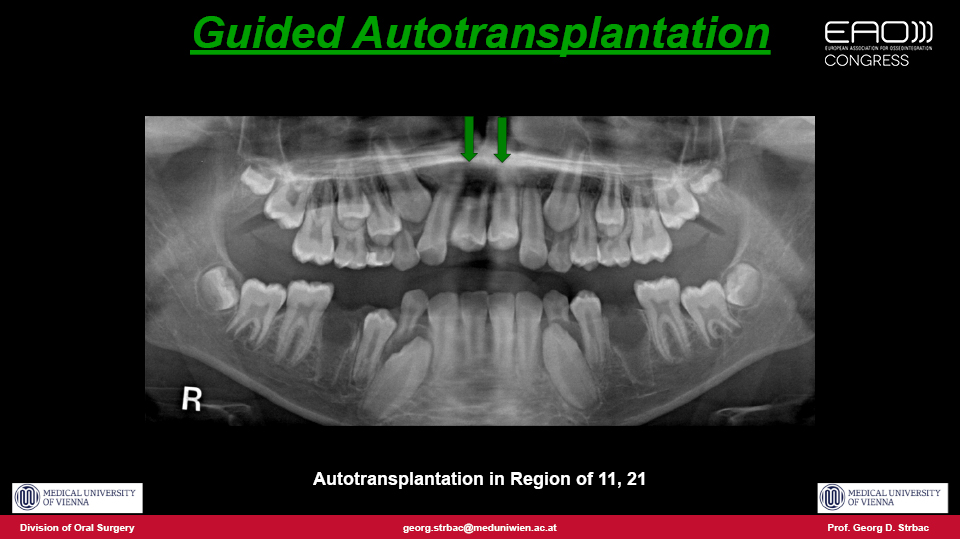
Figure 7

Figure 8

Figure 9

Figure 10

Figure 11
Figure 12
References:
Andreasen JO (ed) Atlas of Replantation and Transplantation of Teeth. Mediglobe SA. Friburg; 1992.
Strbac GD, Giannis K, Mittlböck M, Fuerst G, Zechner W, Stavropoulos A, Ulm C. Survival rate of autotransplanted teeth after 5 years – A retrospective cohort study. J Craniomaxillofac Surg. 2017 Aug;45(8):1143-1149. doi: 10.1016/j.jcms.2017.03.023. Epub 2017 Apr 18.
Strbac GD, Schnappauf A, Giannis K, Bertl MH, Moritz A, Ulm C. Guided Autotransplantation of Teeth: A Novel Method Using Virtually Planned 3-dimensional Templates. J Endod. 2016 Dec;42(12):1844-1850. doi: 10.1016/j.joen.2016.08.021. Epub 2016 Oct 21.
No-prep restorative techniques
No-prep resin-bonded bridges are a well-known option for restoring single-tooth gaps in the anterior region. However, their long-term success remains closely related to proper handling of the material properties, adhesive technique and occlusion. If handled properly, the single-unit, single-retainer cantilever resin-bonded bridge has a definitive role in the treatment of missing front teeth.
To hold the pontic, only a veneer on the palatal side of the adjacent tooth is required (Figures 1–2). The mechanical resistance depends on adhesion to the enamel of the adjacent tooth, and is better when less enamel reduction is required. In short, the less prep done, the more the resistance. No-prep bridges do not weaken the abutment tooth and therefore leave its elastic modulus intact. Regarding materials: the speaker stated that the most frequently used is lithium disilicate, although the use of zirconia is becoming more common.
“The mechanical resistance depends on adhesion to the enamel of the adjacent tooth”
There are a number of clinical situations where resin-bonded all-ceramic cantilever bridges may be properly indicated:
- to replace anterior teeth in children
- cases involving congenitally missing teeth
- cases with retained teeth (such as canines)
- to prevent mesial drifting of molars to the space of a missing tooth by acting as a ‘tilt stopper’
- to replace lower incisors
- immediate cantilever after tooth extraction
- immediate reconstruction after a failed implant
- in patients who have a fear of or aversion to metal
- when price is an issue for the patient
- in patients with aggressive periodontitis
- even in cases involving full mouth rehabilitation
Molar replacement is not recommended with this kind of prosthesis because of mechanical issues. The cantilever would be too distal if used in the posterior region.
It has been observed that mesial contacts of implant crowns which are adjacent to natural teeth tend to open over time (Thilander. 2009; Daftary et al. 2013). With bonded bridges, this did not happen. As the bridge follows the movement of mesial teeth it closes the contact point. The mucosal contact of the pontic can be made to reshape the soft tissue achieving a high pink aesthetic appearance (Figures 3–4).
“The mucosal contact of the pontic can be made to reshape the soft tissue achieving a high pink aesthetic appearance”
The literature shows that single-retainer (cantilever) all-ceramic adhesive bridges perform better than bridges held on two retainers (Kern. 2005; Etemadi et al. 1997), and that single-unit resin-bonded cantilever bridges may perform (clinically) as well as single-unit implants and three-unit bridges with similar OHRQoL results (Lam et al. 2014).
Survival rates over 95% at 5 years and 90% at 10 years have been reported. The two most common complications are fractures and debonding, both of which are easily resolved (Sailer et al. 2013; Botelho et al. 2014; Sasse & Kern. 2014).
“Survival rates over 95% at 5 years and 90% at 10 years have been reported”
The speaker concluded by cautioning that, like most dental procedures, no-prep restorations are technique-sensitive. The rules of material science, adhesive technology and occlusion must be adhered to.
Presentation figures

Figure 1

Figure 2

Figure 3

Figure 4
References:
Botelho MG, Ma X, Cheung GJ, Law RK, Tai MT, Lam WY. Long-term clinical evaluation of 211 two-unit cantilevered resin-bonded fixed partial dentures. J Dent. 2014 Jul;42(7):778-84. doi: 10.1016/j.jdent.2014.02.004. Epub 2014 Mar 28.
Daftary F, Mahallati R, Bahat O, Sullivan RM. Lifelong craniofacial growth and the implications for osseointegrated implants. Int J Oral Maxillofac Implants. 2013 Jan-Feb;28(1):163-9. doi: 10.11607/jomi.2827.
Etemadi S, Smales RJ, Drummond P, Goodhart JR. Australian and New Zealand Division 36th Annual Scientific Meeting, September 29–October 2, 1996 Sydney, Australia. J Dent Res 1997;76(5):936. Abstract no. 14
Kern M. Clinical long-term survival of two-retainer and single-retainer all-ceramic resin-bonded fixed partial dentures. Quintessence Int. 2005 Feb;36(2):141-7.
Lam WY, McGrath CP, Botelho MG. Impact of complications of single tooth restorations on oral health-related quality of life. Clin Oral Implants Res. 2014 Jan;25(1):67-73. doi: 10.1111/clr.12166. Epub 2013 Apr 15.
Sailer I, Bonani T, Brodbeck U, Hämmerle CH. Retrospective clinical study of single-retainer cantilever anterior and posterior glass-ceramic resin-bonded fixed dental prostheses at a mean follow-up of 6 years. Int J Prosthodont. 2013 Sep-Oct;26(5):443-50. doi: 10.11607/ijp.3368.
Sasse M & Kern M. Survival of anterior cantilevered all-ceramic resin-bonded fixed dental prostheses made from zirconia ceramic. J Dent. 2014 Jun;42(6):660-3. doi: 10.1016/j.jdent.2014.02.021. Epub 2014 Mar 5.
Thilander B. Dentoalveolar development in subjects with normal occlusion. A longitudinal study between the ages of 5 and 31 years. Eur J Orthod. 2009 Apr;31(2):109-20. doi: 10.1093/ejo/cjn124.
Discussion
Are there any contraindications for cantilevers? If cantilevers are used cautiously, they can work properly even in patients with bruxism, provided that they are used in incisors and the premolar zone, and are always placed to the mesial side to match the direction of occlusal forces.
Is resorption an unavoidable issue in tooth transplantation? The rate of resorption is about 15%. The fewer injuries in the periodontium, the less resorption we see. That is why a precise pre-treatment plan following a guided osteotomy during autotransplantation is highly recommended in the future.
What is the best way to keep a transplanted tooth in place? Non-rigid methods can keep the tooth fixed in its new position while maintaining slight mobility for the tooth during the healing period. Sutures crossing the occlusal plane are mostly recommended and should be removed after 7–10 days (except in cases involving severe bone defects, where removal should be delayed to 2–3 weeks).
In autotransplantation, is GBR recommended to for improving local conditions? No bone substitutes should be used when transplanting a tooth. The regenerative capacity of the vital periodontium means that substitutes are not needed.
What would you do in a case involving a teenager who had lost an upper central incisor?
- Dr. Romano said he would try to treat the case using autotransplantation. If this approach weren’t possible, he would opt to use orthodontic closure of the space
- Prof. Strbac made it clear that his approach would be autotransplantation without a doubt, bearing in mind that if the autotransplant failed, an implant would still be possible when growth had finished
- Dr. Brodbeck would choose to make a single cantilevered pontic to gain time for the growth to finish