 Watch the webcast
Watch the webcast
 Take-home messages
Take-home messages
 Download summary
Download summary
 Share summary
Share summary



Risks and complications
Reducing risks in implant dentistry
Introduction
Since the field of implant dentistry was first introduced, procedures have been refined and optimised for clinical practice with a view to improving the predictability and reliability of results. Today, our focus is now on preventing and reducing risks.
“Today, our focus is now on preventing and reducing risks”
New approaches have been proposed, such as digital workflows and flapless surgery. However, these come with a number of potential risks which all practitioners should be aware of. For bone regeneration procedures, we need materials which will result in the highest biological activity and the lowest morbidity. However, the potential risk associated with these materials is still under debate and the topic is widely discussed.
Risks for digital work-flow
The trend towards digital workflows in implant dentistry is gaining momentum. This evolution is driven by the desire for simpler, faster, more predictable and more precise treatment methods. But we must dispel the misconception that ‘digital’ is synonymous with ‘infallible’. Errors are still a very real possibility in digital workflows, and there are a number of diverse risks which we should be aware of.
“The trend towards digital workflows in implant dentistry is gaining momentum”
Although errors can arise from every phase of the digital workflow, the speaker focused only on the surgical applications of digital workflows and their associated risks (Figure 1).
“The speaker focused on the surgical applications of digital workflows and their associated risks”
During the ‘data acquisition’ phase, there are three main sources where potential errors might arise: patient movements, metal artefacts or incorrect position of the radiological template. When merging bone data with the information about the final position of the abutments, particular attention should be given to the accuracy of the protocol used and to any software warnings.
When manufacturing the surgical guide, a range of diverse techniques and materials may be used. Significant differences in the precision of these techniques and other associated variables have been observed, but unfortunately there are still no quality standards which have been widely accepted. More research to compare the materials and production techniques of surgical guides is required.
“More research to compare the materials and production techniques of surgical guides is required”
The speaker emphasised that the fit of the guide should always be checked in the patient before treatment, to avoid possible undercuts, check the practicality of the sleeves, and adjust for mouth opening and any changes which might have occurred since the scan was done.
“Before treatment, the surgical guide should always be checked in the patient”
The literature demonstrates that with guided surgery, some deviations between the planned and final implant positions should be expected. We know that:
- tooth-supported guides are the most accurate, compared with bone-supported or mucosal-supported guides
- in free-end cases, some bending of the template will lead to more deviation between the planned and final position; so the less distal implant’s position is, the more accurate the outcome
- as a general rule, when using mucosa-supported guides, the practitioner should allow for a mean 5º angular deviation, which can be minimised by adding fixation pins
Cases involving fully edentulous patients are the most difficult in terms of precisely placing surgical guides and transferring the planned positions of the implants. Several studies using micro-screws have shown improved results (Tahmaseb et al. 2009; Widmann et al. 2010; Mai et al. 2018) (Figure 2). A recent study reported a mean angular deviation of 4.8º and, most importantly, a maximum deviation of almost 15º (Schnutenhaus et al. 2018).
It has been shown that deviations can be reduced from 5º to 2º (± 0.9) (Lee et al. 2016) by using the sleeves close to the bone, with sharp drills and trying to to drill in a centric fashion in order to prevent the deflection of the drill.
A limited mouth opening could also pose a problem, and this should be checked in the patient beforehand. It can be noted that open sleeves require less height. The speaker emphasised that overheating should be prevented by avoiding forceful drilling and ensuring proper cooling.
“Overheating should be prevented by avoiding forceful drilling and ensuring proper cooling”
The intrinsic tolerance of the surgical guide when drilling eccentrically has been investigated in vitro (Van Assche & Quirynen. 2010; Koop et al. 2012). The conclusions were:
- the guide allows an angular deviation of up to 5.2º
- apical deviations are greater than coronal deviations
- deviations increase with depth
- the closer the sleeve is to bone, the less deviation is observed
- higher key holders are associated with less drill deviation
Placing the implants through the sleeves (fully guided) can result in less deviation compared with placing implants free-hand after having drilled with the guide (partially guided) (Bencharit et al. 2018; Younes et al. 2018).
The speaker also cautioned that the guides should be designed with enough space for a flap in order to minimise the amount of keratinised tissue lost by punching (when this approach is indicated).
Another issue which the speaker highlighted is primary stability. It is harder to feel the bone resistance through the guide, and some implants could be loose (‘spinners’). The only way to prevent this is to follow the drilling protocol recommended for soft bone (when indicated) and stop when the implant driver is in place, so as not to turn the implant any more without advancing it.
“Another issue which the speaker highlighted is primary stability”
In summary, a sound understanding of the potential deviations from planned to final implant positions associated with a digital workflow is necessary. An individual risk analysis should always be performed, and a precise and careful treatment approach is the best option for preventing problems and minimising risk.
Presentation figures
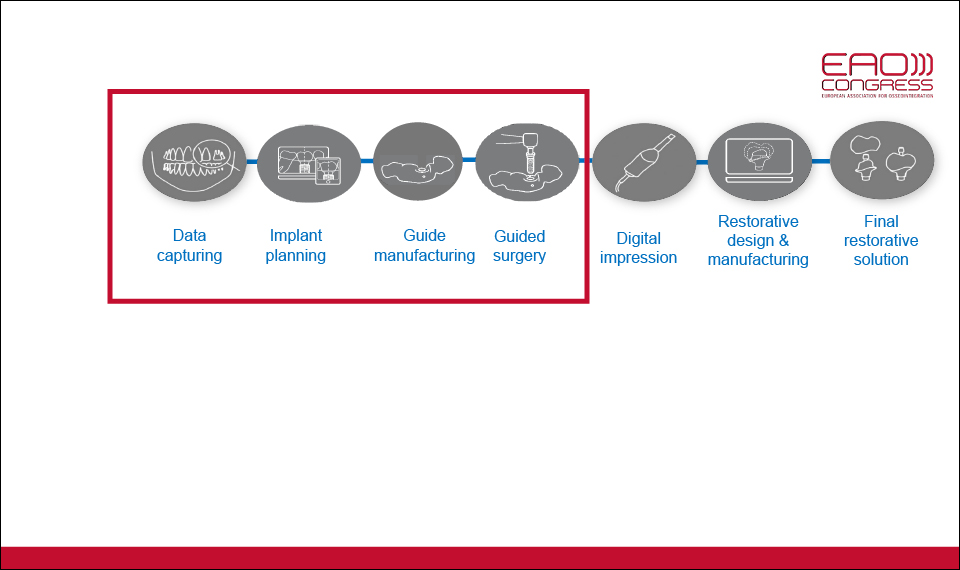
Figure 1
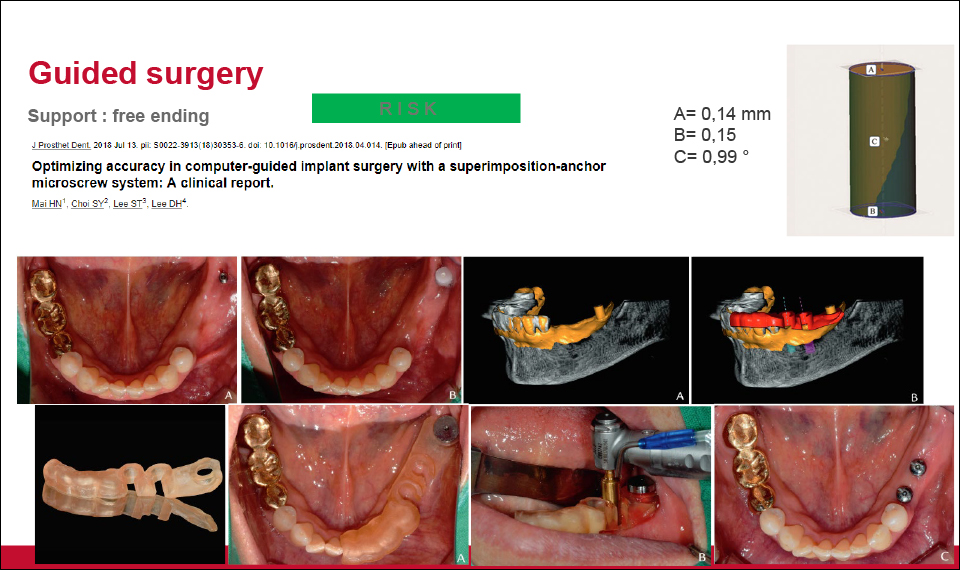
Figure 2
References:
Bencharit S, Staffen A, Yeung M, Whitley D 3rd, Laskin DM, Deeb GR. In Vivo Tooth-Supported Implant Surgical Guides Fabricated With Desktop Stereolithographic Printers: Fully Guided Surgery Is More Accurate Than Partially Guided Surgery. J Oral Maxillofac Surg. 2018 Jul;76(7):1431-1439. doi: 10.1016/j.joms.2018.02.010. Epub 2018 Feb 21.
Koop R, Vercruyssen M, Vermeulen K, Quirynen M. Tolerance within the sleeve inserts of different surgical guides for guided implant surgery. Clin Oral Implants Res. 2013 Jun;24(6):630-4. doi: 10.1111/j.1600-0501.2012.02436.x. Epub 2012 Mar 13.
Lee DH, Mai HN, Yang JC, Kwon TY. The effect of 4,4′-bis(N,N-diethylamino) benzophenone on the degree of conversion in liquid photopolymer for dental 3D printing. J Adv Prosthodont. 2015 Oct;7(5):386-91. doi: 10.4047/jap.2015.7.5.386. Epub 2015 Oct 28.
Mai HN, Choi SY, Lee ST, Lee DH. Optimizing accuracy in computer-guided implant surgery with a superimposition-anchor microscrew system: A clinical report. J Prosthet Dent 2018;120(5):789.e1-e5. doi: https://doi.org/10.1016/j.prosdent.2018.04.014
Schnutenhaus S, Edelmann C, Rudolph H, Dreyhaupt J, Luthardt RG. 3D accuracy of implant positions in template-guided implant placement as a function of the remaining teeth and the surgical procedure: a retrospective study. Clin Oral Investig. 2018 Jul;22(6):2363-2372. doi: 10.1007/s00784-018-2339-8. Epub 2018 Jan 22.
Tahmaseb A, De Clerck R, Wismeijer D. Computer-guided implant placement: 3D planning software, fixed intraoral reference points, and CAD/CAM technology. A case report. Int J Oral Maxillofac Implants. 2009 May-Jun;24(3):541-6.
Van Assche N, Quirynen M. Tolerance within a surgical guide. Clin Oral Implants Res. 2010 Apr 1;21(4):455-8. doi: 10.1111/j.1600-0501.2009.01836.x. Epub 2010 Jan 13.
Widmann G, Zangerl A, Keiler M, Stoffner R, Bale R, Puelacher W. Flapless implant surgery in the edentulous jaw based on three fixed intraoral reference points and image-guided surgical templates: accuracy in human cadavers. Clin Oral Implants Res. 2010 Aug;21(8):835-41. doi: 10.1111/j.1600-0501.2009.01884.x. Epub 2010 Mar 25.
Younes F, Cosyn J, De Bruyckere T, Cleymaet R, Bouckaert E, Eghbali A. A randomized controlled study on the accuracy of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients. J Clin Periodontol. 2018 Jun;45(6):721-732. doi: 10.1111/jcpe.12897. Epub 2018 May 10.
Risks for flapless surgery
Although reflecting a muco-periosteal flap is still considered the gold standard for placing implants, the flapless approach is becoming increasingly recommended as a minimally invasive surgical option. There are three ways of performing flapless surgery:
- immediate post-extraction placement
- punch flap
- trans-gingival approach
The approach which involves raising a flap provides good bone visibility, safer distribution of keratinised tissues and allows the possibility of grafting. However, this approach is also associated with longer surgical times, postoperative inflammation and crestal bone resorption.
“The flapless approach is becoming increasingly recommended as a minimally invasive surgical option”
In cases involving fresh extraction sockets, flapless implant placement is highly recommended since it seems to be the best way to maintain tissue morphology. But this too is not without its disadvantages: it is harder to see apical lesions or remove granulation tissues, and it is not possible to augment the contour of the ridge with the flapless approach (Cosyn et al. 2012).
Regarding punch and trans-gingival approaches, only limited and short-term benefits for postoperative healing have been reported compared with open flap surgery (Aizenberg et al. 2013). Punching needs a large amount of bone volume and wide gingiva, since it removes about 5mm of keratinised tissue. Both punching and trans-gingival approaches have limited visibility of bone topography, and they are both associated with a risk of intrabony contamination by bacteria, epithelium or connective tissue.
“Both punching and trans-gingival approaches have limited visibility of bone topography”
A meta-analysis comparing flap and flapless approaches found no significant differences between the rates of implant failures (Chrcanovic et al. 2014). This could be due to insufficient statistical power or the presence of confounding factors (grafting, extraction sockets, guided surgery, etc.). Another more recent meta-analysis revealed that flapless procedures may increase the risk of implant failures, especially when loaded with immediate or early approaches. Nevertheless, it was reported that flapless procedures preserved bone tissues better and were associated with lower levels of bone resorption (Zhuang et al. 2018).
Since the flapless procedure is a ‘blind’ surgical technique (meaning that the underlying bone anatomy remains unseen), the risk of perforating the cortical plates increases, as does the risk of placing implants outside the bony envelope. Even in the case of guided flapless procedures, the risk of perforation persists due to the unavoidable deviations which occur during guided surgery. Navigation has been proposed as a way of performing flapless surgery with fewer risks, but this technology is currently too complex and too expensive to be widely utilised.
“The flapless procedure is a ‘blind’ surgical technique”
Flapless approaches should only be indicated in cases where conditions are suitable, with ‘good bone and good gingiva’.
The speaker stated that the risks associated with the procedure can be safely managed only after a proper and individualised treatment plan is drawn up. To emphasise this, they quoted the saying: ‘failing to plan is planning to fail’.
References:
Aizenberg A, Jansson J, Abrahamsson P. jShort-term postoperative discomfort in patients receiving flapless contra open implant surgery. Open J Stomatol, 2013;3:298-305. doi:10.4236/ojst.2013.35050
Chrcanovic BR, Albrektsson T, Wennerberg A. Flapless versus conventional flapped dental implant surgery: a meta-analysis. PLoS One. 2014 Jun 20;9(6):e100624. doi: 10.1371/journal.pone.0100624. eCollection 2014.
Cosyn J, Hooghe N, De Bruyn H. A systematic review on the frequency of advanced recession following single immediate implant treatment. J Clin Periodontol. 2012 Jun;39(6):582-9. doi: 10.1111/j.1600-051X.2012.01888.x. Epub 2012 Apr 18.
Zhuang J, Zhao D, Wu Y, Xu C. Evaluation of Outcomes of Dental Implants Inserted by Flapless or Flapped Procedure: A Meta-Analysis. Implant Dent. 2018 Oct;27(5):588-598. doi: 10.1097/ID.0000000000000820.
Risks for bone substitute materials
To achieve optimal results, 40% of cases require augmentative procedures before implants are placed. In the aesthetic zone, this figure increases to 90%.
The risks associated with bone augmentation depend on a number of factors, most of which are more relevant than the properties of the bone regeneration materials used. These factors include: the immunological status and systemic diseases of the patient; the patient’s compliance, oral hygiene and lifestyle; the morphology of the defect; the bone quantity and quality; and the type of implant treatment (immediate placement, loading, etc.) being utilised.
“The risks associated with bone augmentation depend on a number of factors, most of which are more relevant than the material itself”
What are the limiting factors in peri-implant regeneration?
- simultaneous regeneration of bone and soft tissue
- presence of oral biofilm
- regeneration on a hard, non-vascularised surface
- the pressure put on mechanical loading during mastication
The patient’s condition should be taken into account, as the wound healing process may be compromised as a result of:
- a history of periodontitis
- diabetes mellitus
- irradiation
- anti-resorptive medication
- smoking
- previous implant failures
Peri-implant tissues have fewer hemidesmosomes and lower levels of perfusion compared to natural teeth. Peri-implant regeneration must be carried out in a hypovascular and hypocellular tissue. There are many techniques which could be used to achieve this, but 90% of the graft’s nutrition comes from the periosteum, and this has to be split to allow flap extension. The speaker outlined a formula for ensuring success: making sure there is adequate space for bone to grow and raising a tension-free flap.
In order to improve the interaction with bone, bone regeneration materials (BRM) are manufactured to be similar to human bone. They show: an interconnecting pore system, a neutral pH and an appropriate resorption rate for bone healing (Kolk et al. 2012).
It is becoming increasingly common for allograft materials to be harvested from living donors, especially from coxarthrosis patients. Allogeneic bone can be considered a reliable alternative with minimal morbidity, due to the reported low failure rates in the maxilla – 2.4% (Monje et al. 2014) – and an implant survival rate of 95.3% in the mandible (Nissan et al. 2011).
“It is becoming increasingly common for allograft materials to be harvested from living donors”
Not all risks can be eliminated. In theory, however, 1:10 of potential infections are covered by the product’s company liability insurance (Nissan et al. 2011). Decellularisation cannot be ensured in 100% of cases. Although small traces of DNA remains can be found, they have been shown to not have any antigenicity. It is recommended that this theoretical risk be included in the patient pre-operative information, although there have been no documented cases in the dental field. Current legal regulations only require that origin, sterility and traceability data are included when using allografts.
Most synthetic bone substitutes are denser than allogeneic bone, and do not have an interconnected structure with similar pore size and distribution to cancellous bone, as allogeneic bone does (Klein et al. 2009). It has been shown that synthetic bone substitutes are incapable of vascular ingrowth, and elicit more fibrous tissue. Larger pores, with a diameter of about 400–600µ, have been reported to better promote blood vessel formation (Ghanaati et al. 2013). The osteoconductivity of bone substitutes is determined by bone-like pore structures.
“Although not all risks can be eliminated, allogeneic bone can be currently considered to be safe”
The main problem associated with autogenous and allogeneic bone is rapid resorption. Because of this, it is recommended that they be supplemented with a mix of xenografts or alloplasts, using less than 50% of the ratio (usually around 25% of bone substitutes). The more the patient’s local and general condition deviates from the ideal situation (i.e. the riskier their situation is), the higher the proportion of autogenous bone can be used.
Before augmentation procedures are performed, a risk analysis should be carried out to identify: anticoagulants, anti-resorptive medications, any immunodeficiency conditions or irradiation. the German Association of Oral Implantology (DGI) has a risk-evaluation sheet for implants in patients taking anti-resorptive drugs (www.dginet.de/web/dgi/laufzettel-bisphosphonate).
References:
Ghanaati S, Barbeck M, Lorenz J, Stuebinger S, Seitz O, Landes C, Kovács AF, Kirkpatrick CJ, Sader RA. Synthetic bone substitute material comparable with xenogeneic material for bone tissue regeneration in oral cancer patients: First and preliminary histological, histomorphometrical and clinical results. Ann Maxillofac Surg. 2013 Jul;3(2):126-38. doi: 10.4103/2231-0746.119221.
Klein M, Goetz H, Pazen S, Al-Nawas B, Wagner W, Duschner H. Pore characteristics of bone substitute materials assessed by microcomputed tomography. Clin Oral Impl Res. 2009;20:67–74. doi: 10.1111/j.1600-0501.2008.01605.x
Kolk A, Handschel J, Drescher W, Rothamel D, Kloss F, Blessmann M, Heiland M, Wolff KD, Smeets R. Current trends and future perspectives of bone substitute materials – from space holders to innovative biomaterials. J Craniomaxillofac Surg. 2012 Dec;40(8):706-18. doi: 10.1016/j.jcms.2012.01.002. Epub 2012 Jan 31.
Monje A, Pikos MA, Chan HL, Suarez F, Gargallo-Albiol J, Hernández-Alfaro F, Galindo-Moreno P, Wang HL. On the feasibility of utilizing allogeneic bone blocks for atrophic maxillary augmentation. Biomed Res Int. 2014;2014:814578. doi: 10.1155/2014/814578. Epub 2014 Sep 11.
Nissan J, Ghelfan O, Mardinger O, Calderon S, Chaushu G. Efficacy of cancellous block allograft augmentation prior to implant placement in the posterior atrophic mandible. Clin Implant Dent Relat Res. 2011 Dec;13(4):279-85. doi: 10.1111/j.1708-8208.2009.00219.x. Epub 2009 Aug 5.
https://www.dginet.de/web/dgi/laufzettel-bisphosphonate Authors: Grötz KAS and Al-Nawas B.