 Watch the webcast
Watch the webcast
 Take-home messages
Take-home messages
 Download summary
Download summary
 Share summary
Share summary



Managing cases
Management of highly atrophic cases
Introduction
Highly atrophic jaws continue to pose a great challenge in implant dentistry. There are still no definite solutions for rehabilitating these cases, since there is no general consensus regarding treatment.
“Highly atrophic jaws continue to pose a great challenge in implant dentistry. “
The chairs outlined several questions which would be addressed in the following presentations and discussion:
- in which cases should we decide to regenerate, and in which ones should we use short or narrow-diameter implants?
- what surgical techniques are available for reconstructing atrophic ridges?
- what is the longevity of short implants versus that of vertical augmentation?
- what is the minimum amount of bone needed to place a narrow-diameter implant?
- what is the maximum depth at which we can place a short implant between natural teeth?
- what is the scientific evidence supporting the answers to these questions?
Ridge augmentation procedures
In implant dentistry, the aim of bone augmentation is not merely to achieve osseointegration, but to improve function and aesthetics (evidence type III: based on clinicians’ experience). Bone atrophy in the jaw presents an important functional and aesthetic dilemma. The clinician must make the decision to rebuild the lost volume using bone augmentation procedures or make a compromise on the prosthetic solution.
“Bone atrophy in the jaw presents an important functional and aesthetic dilemma. “
Sufficient bone volume is a key factor for implant health. But the main problem associated with bone grafting is morbidity. Current bone augmentation solutions tend to favour patient-friendly and minimally invasive techniques, for example:
- making a minimal-access incision in the iliac crest and harvesting a autologous graft using the ‘piano keys’ technique
- using biomaterials in interpositional grafting procedures such as the ‘sandwich’ technique
“Sufficient bone volume is a key factor for implant health.”
It is widely accepted in the literature (evidence type II) that interpositional grafts are safer and are associated with less resorption than onlay grafts (Stellingsma et al. 2014; Troeltzsch et al. 2016). The positioning of an onlay graft on top of the ridge leads to pulling and stretching of the soft tissue, and soft tissue augmentation is often required. Whereas soft tissue work is not necessary in the interpositional technique, as the soft tissue stays on top of the crest and is not detached, and thus passively follows the bone.
“It is widely accepted that interpositional grafts are safer than onlay grafts”
The speaker described a 4mm threshold for vertical augmentation. This is probably due to the fact that angiogenesis does not come further than 3 or 4mm out of the bone envelope. Interpositional grafts have an advantage in that they have 4mm from the vascularised top, and 4mm from the bottom, and therefore double the source of angiogenesis.
References:
Stellingsma K, Raghoebar GM, Visser A, Vissink A, Meijer HJ. The extremely resorbed mandible, 10-year results of a randomized controlled trial on 3 treatment strategies. Clin Oral Implants Res. 2014 Aug;25(8):926-32. doi: 10.1111/clr.12184. Epub 2013 May 3.
Troeltzsch M, Troeltzsch M, Kauffmann P, Gruber R, Brockmeyer P, Moser N, Rau A, Schliephake H. Clinical efficacy of grafting materials in alveolar ridge augmentation: A systematic review. J Craniomaxillofac Surg. 2016 Oct;44(10):1618-1629. doi: 10.1016/j.jcms.2016.07.028. Epub 2016 Aug 18.
Short and reduced diameter implants
There is currently a global trend towards the use of minimally invasive procedures, and it is perhaps the most discussed topic in the field of implant dentistry.
In cases where limited bone is available (both in terms of width and depth), there is the option of using short and small-diameter implants instead of bone augmentation, which are associated with morbidity and potential risk of complications.
In the 1st EAO Consensus Conference in 2006, short implants were defined as a device with a designed intra bony length of ≦ 8mm and narrow implants as one in which the stated diameter was ≦ 3.5mm (Renouard & Nisand. 2006). It was also pointed out that short and narrow implants are mostly used in cases involving reduced bone volume and must therefore be compared to standard implants associated with bone augmentation procedures.
“Bone augmentation was associated with greater morbidity than short and narrow implants.”
Where are we now?
The most recent systematic reviews comparing short implants with standard implants plus bone augmentation (Nielsen et al. 2018; Pommer et al. 2016; Tolentino et al. 2018; Palacios et al. 2017; Dias et al. 2018; Starch-Jensen et al. 2017; Uehara et al. 2018; Rokn et al. 2018) had the following conclusions:
- implant and reconstruction survival rates are similar in both options
- short implants have favourable treatment time, cost, morbidity and patient-related outcomes
However, more long-term follow-up clinical studies are needed (ten years post-loading). Further investigation of the impact of implant diameter and the design of prosthetic reconstructions on the survival rate is also recommended.
“Short implants have favourable treatment time, cost, morbidity and patient-related outcomes”
Although several clinical studies have used narrow-diameter implants in almost all clinical scenarios, RCTs comparing them with standard implants (plus lateral bone augmentation) are still lacking.
As a consequence, there is currently insufficient evidence-based information and clinical recommendations for the indication of narrow-diameter implants in posterior zones with reduced bone volume.
“However, more long-term follow-up clinical studies are needed”
Compared to standard implants, short and narrow-diameter implants seem to behave similarly regarding peri-implantitis and prosthetic complications. On the other hand, very scarce data is available regarding the behaviour of implants placed in augmented bone with respect to peri-implantitis.
The key factors for preventing biological complications are: prosthetically driven implant placement, and soft tissue management to ensure adequate thickness of keratinised tissue.
Presentation figures
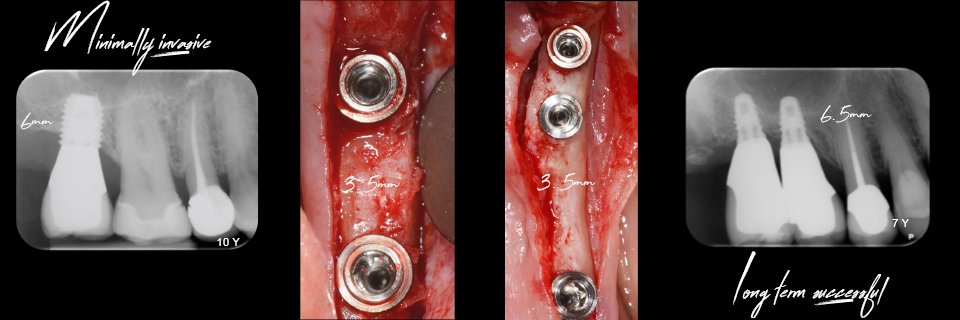
Figure 1

Figure 2
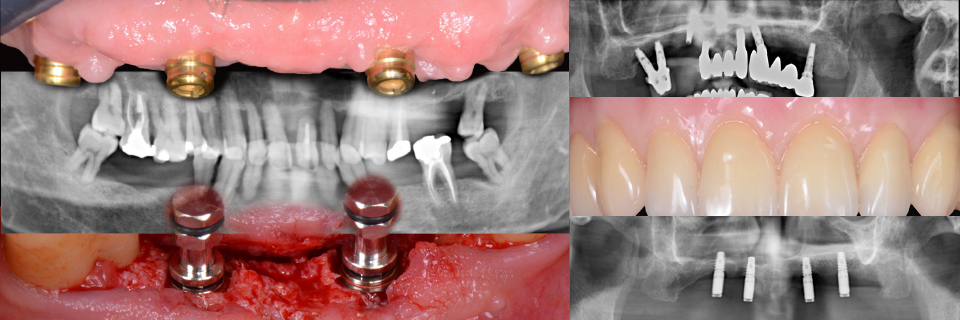
Figure 3
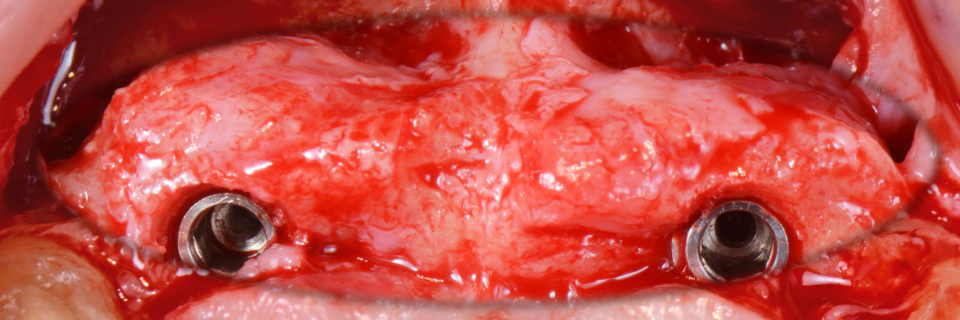
Figure 4
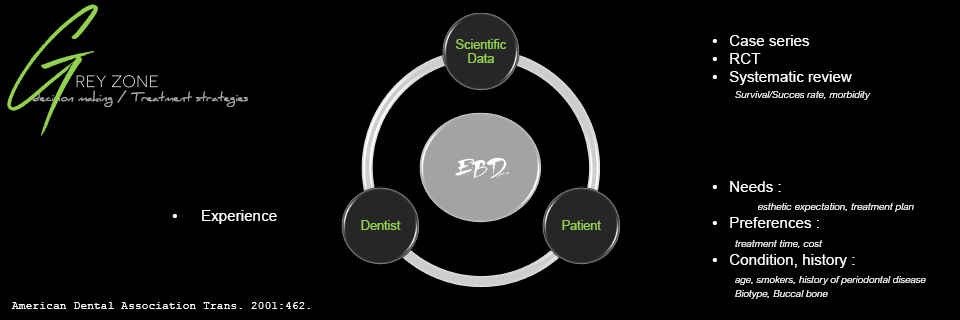
Figure 5

Figure 6
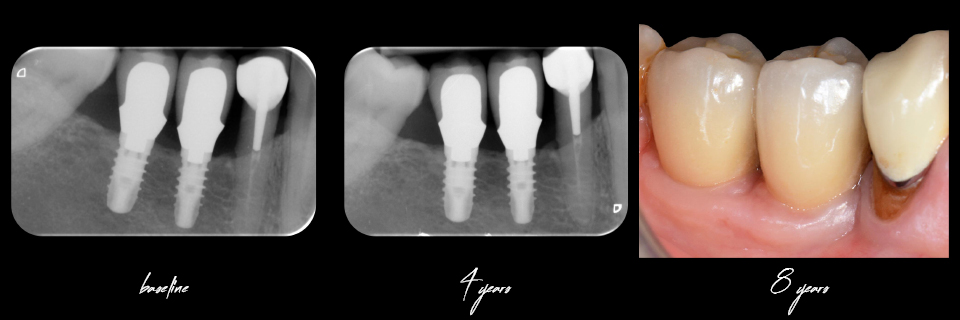
Figure 7
Figure 8
References:
Dias, FJ de N, Pecorari VGA, Martins CB, Del Fabbro M, Casati MZ. Short implants versus bone augmentation in combination with standard-length implants in posterior atrophic partially edentulous mandibles: systematic review and meta-analysis with the Bayesian approach. Int J Oral Maxillofac Surg 2019;48(1):90-6.
Klein MO, Schiegnitz E, Al-Nawas B. Systematic review on success of narrow-diameter dental implants. Int J Oral Maxillofac Implants. 2014;29 Suppl:43-54. doi: 10.11607/jomi.2014suppl.g1.3.
Nielsen HB, Schou S, Isidor F, Christensen AE, Starch-Jensen T. Short implants (≤8mm) compared to standard length implants (>8mm) in conjunction with maxillary sinus floor augmentation: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2019 Feb;48(2):239-249. doi: 10.1016/j.ijom.2018.05.010. Epub 2018 Jul 3.
Ortega-Oller I, Suárez F, Galindo-Moreno P, Torrecillas-Martínez L, Monje A, Catena A, Wang HL. The influence of implant diameter on its survival: a meta-analysis based on prospective clinical trials. J Periodontol. 2014 Apr;85(4):569-80. doi: 10.1902/jop.2013.130043. Epub 2013 Aug 1.
Palacios JAV, Garcia JJ, Caramês JMM, Quirynen M, da Silva Marques. Short implants versus bone grafting and standard-length implants placement: a systematic review. Clin Oral Investig. 2018 Jan;22(1):69-80. doi: 10.1007/s00784-017-2205-0. Epub 2017 Oct 6.
Pommer B, Busenlechner D, Fürhauser R, Watzek G, Mailath-Pokorny G, Haas R. Trends in techniques to avoid bone augmentation surgery: Application of short implants, narrow-diameter implants and guided surgery. J Craniomaxillofac Surg. 2016 Oct;44(10):1630-1634. doi: 10.1016/j.jcms.2016.08.012. Epub 2016 Aug 21.
Pommer B, Mailath-Pokorny G, Haas R, Buseniechner D, Millesi W, Fürhauser R. Extra-short (< 7 mm) and extra-narrow diameter (< 3.5 mm) implants: a meta-analytic literature review. Eur J Oral Implantol. 2018;11 Suppl 1:S137-S146.
Renouard F, Nisand D. Impact of implant length and diameter on survival rates. Clin Oral Implants Res. 2006 Oct;17 Suppl 2:35-51.
Rokn AR, Keshtkar A, Monzavi A, Hashemi K, Bitaraf T. Comparing Short Dental Implants to Standard Dental Implants: Protocol for a Systematic Review. JMIR Res Protoc. 2018 Jan 18;7(1):e16. doi: 10.2196/resprot.8836.
Starch-Jensen T, Schou S. Maxillary Sinus Membrane Elevation With Simultaneous Installation of Implants Without the Use of a Graft Material: A Systematic Review. Implant Dent. 2017 Aug;26(4):621-633. doi: 10.1097/ID.0000000000000617.
Tolentino da Rosa de Souza P, Binhame Albini Martini M, Reis Azevedo-Alanis L. Do short implants have similar survival rates compared to standard implants in posterior single crown?: A systematic review and meta-analysis. Clin Implant Dent Relat Res. 2018 Oct;20(5):890-901. doi: 10.1111/cid.12634. Epub 2018 Jul 27.
Uehara PN, Matsubara VH, Igai F, Sesma N, Mukai MK, Araujo MG. Short Dental Implants (≤7mm) Versus Longer Implants in Augmented Bone Area: A Meta-Analysis of Randomized Controlled Trials. Open Dent J. 2018 Apr 30;12:354-365. doi: 10.2174/1874210601812010354. eCollection 2018.
Open questions
How much bone is needed around implants in the posterior (non-aesthetic) region? Is the rule of 1mm bone surrounding the implant neck scientifically based? Is the idea of stress concentration 3mm around the implant neck supported by anything other than finite element analysis?
How far can we go with extra-short, extra-narrow implants and their combined use? Can we safely use extra-short implants in the posterior region? Is there enough evidence for that?
How do we make the decision whether to use short/narrow implants or standard implants on a augmented ridge?
Clinical cases
Hendrik Terheyden
Prof Terheyden presented two cases involving extreme atrophy in totally edentulous patients. The first case was treated with a mandibular sandwich osteotomy filling the interpositional space with biomaterials. In the maxilla, a Le Fort I osteotomy was performed, the pre-maxilla was advanced and bone ‘piano pieces’ from the iliac crest were interpositionally grafted. Standard implants were then placed and two overdentures were secured.
The second case was treated with a Le Fort I osteotomy rebuilding the maxilla using interpositional and onlay grafts. A fixed prosthesis on eight implants was finally placed.
David Nisand
In the anterior region, Dr Nisand recommended bone augmentation to achieve successful long-term aesthetic outcomes. In the posterior region, when the available bone allows for a graftless solution, the use of short and narrow-diameter implants should be considered to simplify treatment. The decision should be based on a thorough case evaluation taking the patient’s specifications and wishes into account. In cases involving extreme atrophy (such as less than 5mm of mandibular bone above the nerve or 3mm residual bone below the sinus) guided bone regeneration should always be implemented to allow for the placement of standard implants.
“In cases involving extreme atrophy guided bone regeneration should always be implemented”
The first case was relatively straightforward: the patient was taking bisphosphonates and the decision was made (according to patient’s condition and their preferences) to place a combination of short and narrow-diameter implants instead of a staged or simultaneous bone augmentation.
The second case involved a female smoker with ongoing periodontitis and peri-implantitis. Aetiological treatment allowed for periodontal treatment along with removal of implants in the posterior zone causing advanced vertical bone defect.
Again, in the context of an all-encompassing treatment plan, the patient’s condition and preferences contributed to the decision to place short implants in the posterior mandible. This was aimed to provide a simpler solution for her and to help the retention of a partial removable denture. Short and narrow implants are indicated in elderly and medically compromised patients.
“Short and narrow implants are indicated in elderly and medically compromised patients.”
For normal patients, they can also provide a faster and cheaper alternative. But three objectives must be fulfilled:
- patient evaluation, to guide them to an evidence-based decision
- correct 3D position for implants
- perio-friendly restoration design
Discussion
It is important to remember that for each defect we encounter, there is an appropriate technique to treat it. We should have no doubts about the quality of regenerated bone, as it is the same as pristine bone. After the bone remodelling process, the grafted materials will, over time, become the patient’s bone.
The most important (and most difficult) step of bone augmentation is to maintain full soft tissue coverage. For traditional augmentation methods, this could be problematic because of the large amount of soft tissue mobilisation which is required to cover the augmented volume without tension. However, current interpositional approaches make it much easier to handle soft tissues. The speakers emphasised that for a safe application of the technique, 5mm of bone above the nerve is needed.
“The most important step of bone augmentation is to maintain full soft tissue coverage”
A short implant is now considered 6mm long; an extra-short implant measures 5–4mm. An 8mm implant is considered a standard-length implant (Figures 1-2).
When using narrow-diameter implants we have to make some prosthetic compromises, and the prosthesis design can be affected. There is a limited number of situations which can be solved with these types of implants in the posterior zone.
“An 8mm implant is now considered a standard-length implant.”
The speakers presented a case involving extreme atrophy in the posterior quadrant of the mandible. This could not be treated with anything other than regeneration. This raised the question: how much bone is needed to safely place short implants? And when should we decide to use regeneration? The speakers explained that at least 7mm (or better, 8mm) of bone should be present above the nerve, and the security margin should measure between 1–2mm. So the case presented did not have enough bone for interpositional grafting or for short implants. The suitable option would be vertical GBR and onlay bone grafting. It should be noted that the limits of these techniques could be estimated at about 4–6mm on average. Should more volume be needed, the approach would require the use of onlay bone blocks. Although in the final decision of what treatment method to undertake, the experience and skill of the surgeon should often be the deciding factor.
A second case was presented (Figures 3-4), involving a knife-edge posterior mandibular crest. A question was raised about the minimum width of bone required to place a narrow-diameter implant. The speakers agreed that 4mm should be the minimum. In the case of a 3mm-wide crest, lateral GBR was recommended with or without simultaneous placement of implants. Splitting was also discussed as an option when little corticalisation is present.
“The experience and skill of the surgeon should often be the deciding factor”
Another challenging situation which was discussed is that of deep bone defects between teeth in the anterior region. Again, it was clearly stated that short implants should be considered in the posterior zone and not in the aesthetic area (Figure 5).
“Short implants should be considered in the posterior zone and not in the aesthetic area”
Although these cases could be treated with short implants, the deep trough created would be difficult to maintain and the sloped spaces between implants and neighbouring teeth could be prone to forming deep pockets. So rebuilding the bone volume first and then creating a proper soft tissue margin to ensure long-term peri-implant health is recommended.
Presentation figures

Figure 1
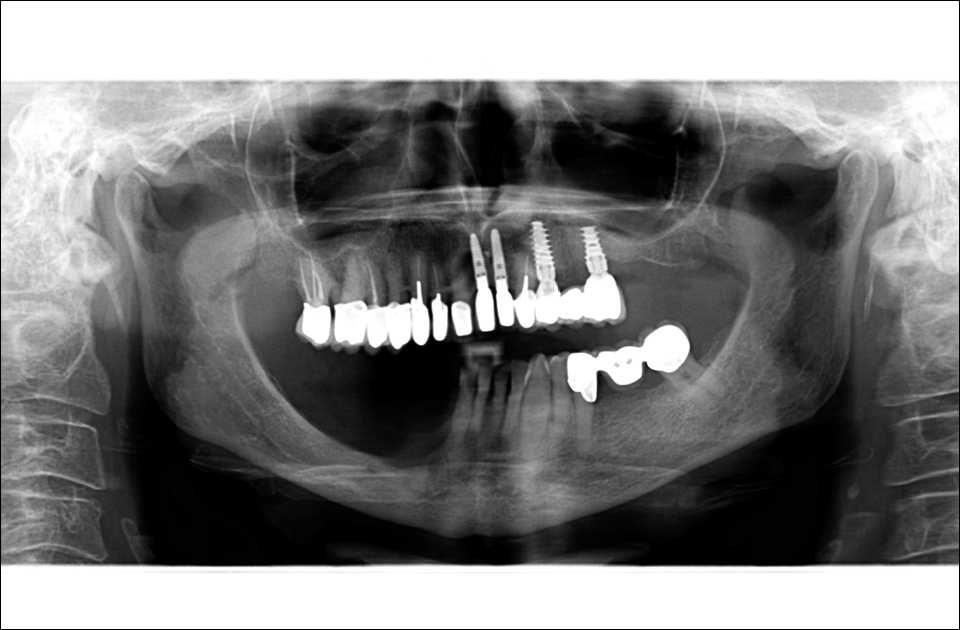
Figure 2

Figure 3
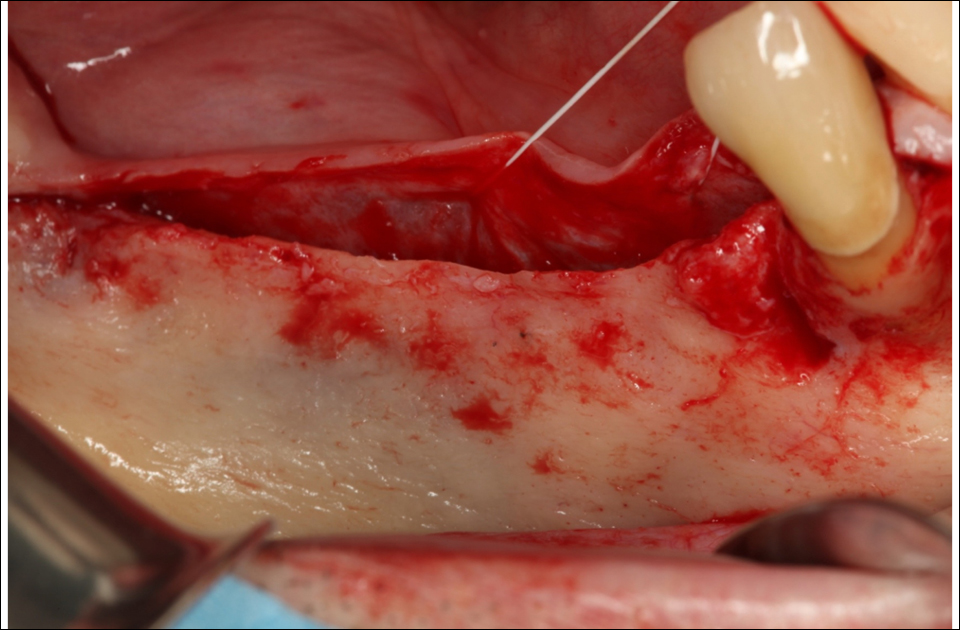
Figure 4

Figure 5